
Clinical Vignette
SM is a 16-year-old right-handed female volleyball player with no significant medical history who presents with progressively worsening right shoulder pain localized to the right periscapular region. There is no associated trauma or inciting event and pain is exacerbated when she serves or spikes the ball, and typically alleviated with rest. She denies any neck pain, radicular symptoms in the arm, or focal weakness, but her right arm just feels weaker, with less velocity on her serve.
Treatment has included rotator cuff strengthening exercises and modalities under the supervision of her athletic trainer, but no physical therapy or injections. She was evaluated by her PCP, who ordered routine x-rays of the right shoulder that were normal. She also states that her PCP noticed her right shoulder blade was sticking out a little, so she underwent an electrodiagnostic evaluation that was negative.
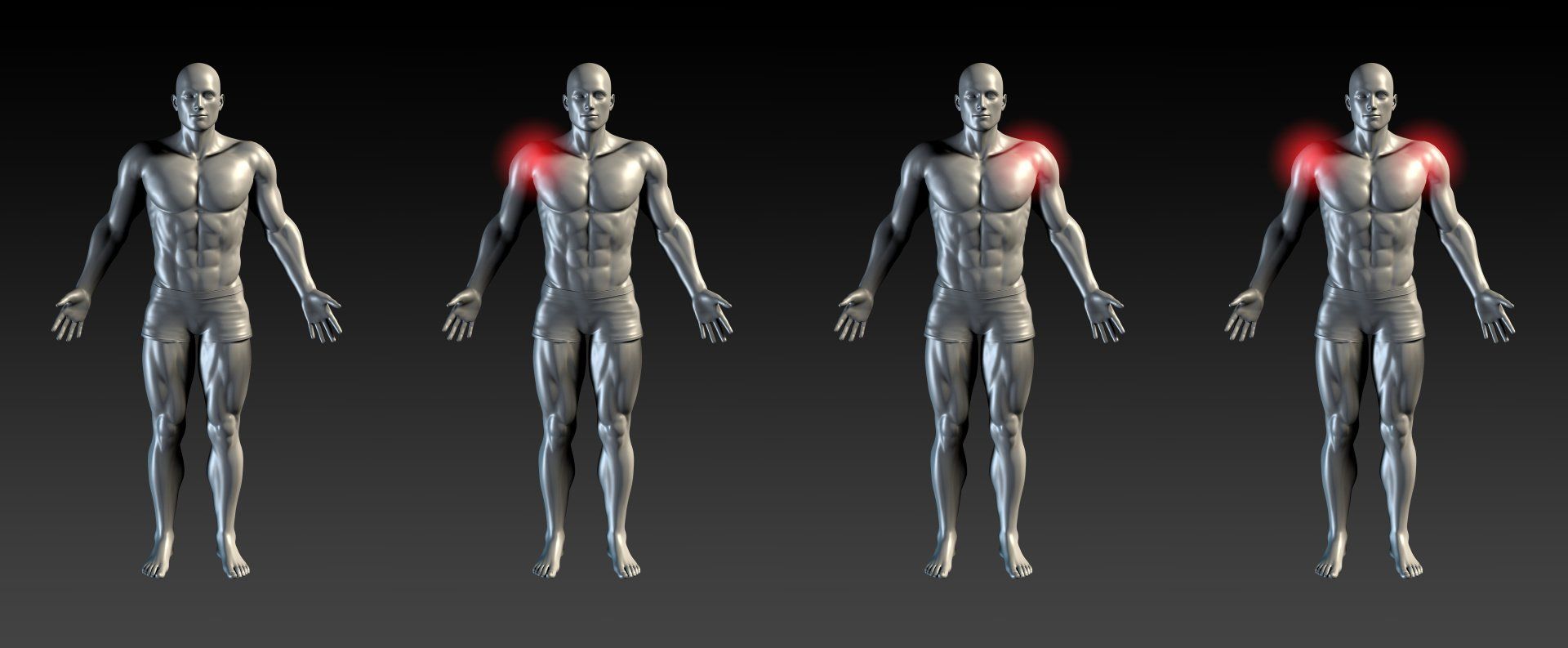
Upon examination at the UPMC Sports and Spine Clinic, she demonstrates slightly increased cervical flexion and forward rounded shoulders. The right scapula is malpositioned with increased prominence of the infero-medial angle. She has full active shoulder range of motion with the exception of pain-limited abduction to 130 degrees and
flexion to 150 degrees (see Figures 2a, 2b, 2c, above). She is tender to palpation along the medial border of the coracoid
process, but otherwise there is no tenderness in the shoulder or cervical spine. Her neurologic and musculoskeletal examination is otherwise unremarkable, with the exception of decreased right hip internal ROM. She is frustrated because she doesn’t know what is wrong and all tests to date have been normal. Now with the volleyball season over, she is looking forward to playing spring softball as an outfielder and is asking for recommendations.
Click hereto download the complete paper.
SM is a 16-year-old right-handed female volleyball player with no significant medical history who presents with progressively worsening right shoulder pain localized to the right periscapular region. There is no associated trauma or inciting event and pain is exacerbated when she serves or spikes the ball, and typically alleviated with rest. She denies any neck pain, radicular symptoms in the arm, or focal weakness, but her right arm just feels weaker, with less velocity on her serve.
Treatment has included rotator cuff strengthening exercises and modalities under the supervision of her athletic trainer, but no physical therapy or injections. She was evaluated by her PCP, who ordered routine x-rays of the right shoulder that were normal. She also states that her PCP noticed her right shoulder blade was sticking out a little, so she underwent an electrodiagnostic evaluation that was negative.
Upon examination at the UPMC Sports and Spine Clinic, she demonstrates slightly increased cervical flexion and forward rounded shoulders. The right scapula is malpositioned with increased prominence of the infero-medial angle. She has full active shoulder range of motion with the exception of pain-limited abduction to 130 degrees and
flexion to 150 degrees (see Figures 2a, 2b, 2c, above). She is tender to palpation along the medial border of the coracoid
process, but otherwise there is no tenderness in the shoulder or cervical spine. Her neurologic and musculoskeletal examination is otherwise unremarkable, with the exception of decreased right hip internal ROM. She is frustrated because she doesn’t know what is wrong and all tests to date have been normal. Now with the volleyball season over, she is looking forward to playing spring softball as an outfielder and is asking for recommendations.
Click hereto download the complete paper.

The baseball and medical communities have recognized injuries of the upper extremity associated with the overhead throwing motion and have examined manners in which to reduce risk.